Familial Colorectal Cancers - Familial Adenomatous Polyposis (FAP)
Table of Contents
About 153,000 people are diagnosed with colorectal cancer each year in the United States. About 10 to 15% of these cancers may be caused by genetic abnormalities that run in families (passed down from your parents). One of these abnormalities is familial adenomatous polyposis (FAP).
FAP is very rare and causes less than one percent of new colorectal cancer cases each year. The average onset of polyps in patients with FAP is age 16. Those with FAP can have hundreds to thousands of adenomatous polyps and have a very high risk of being diagnosed with colorectal cancer by age 40 if they do not have their colon removed.
Adenomatous polyps are called "pre-cancerous" lesions, and it is likely that some will turn into cancer. The more polyps you have, the higher your risk of colorectal cancer. The average age of a colorectal cancer diagnosis in those with FAP is 39 years. It is 72 years for those without FAP.
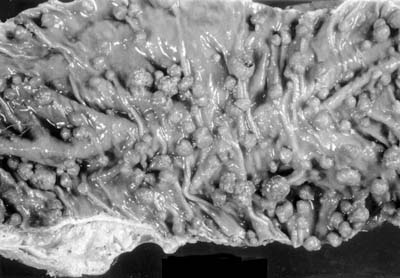
Colon with multiple adenomas, Photo courtesy of Zane Cohen Centre for Digestive Disorders, Mt. Sinai Hospital, Toronto, Canada.
FAP can also increase your risk of stomach, small intestine, pancreatic, biliary tree, hepatoblastoma, medulloblastoma, and papillary thyroid cancers. FAP can also lead to other non-cancerous issues:
- Fibromas and cysts on the skin of the face, scalp, arms, and legs.
- Some will have a freckle in their eye retina called congenital hypertrophy of the retinal pigment epithelium (CHRPE). A person with FAP will likely have it in both eyes, a person who does not have FAP often has it in one eye.
- Dental issues, like extra or missing teeth, fused roots, or non-cancerous tumors of the jaw bone.
- Osteomas (bony growths) in the jaw.
- Masses in the adrenal glands (small glands on top of your kidneys).
- Desmoid tumors which are non-cancerous, slow-growing tumors in the abdomen (belly). They can cause health issues when they press against nearby organs and tissues.
If you have any of these health issues you should talk to your provider about being tested for FAP.

Congenital hypertrophy of the retinal pigment epithelium, Photo courtesy of Zane Cohen Centre for Digestive Disorders, Mt. Sinai Hospital, Toronto, Canada.
Genetics and Screening
The gene that causes FAP is called the Adenomatous Polyposis Coli, or APC gene. There are over 300 different mutations (changes) in the APC gene which can cause FAP. Where the mutation is on the gene is often related to the number of polyps, age of onset, and other factors. FAP is an autosomal dominant inherited disorder. This means a child who has a parent with the affected gene has a 50% chance of inheriting the mutation. Up to 1 out of 3 people with FAP have "de novo mutations," meaning they have no family history of the mutation.
The diagnosis of FAP is made when you have more than 100 adenomatous polyps found during a colonoscopy or when genetic testing is done in a family with a history of FAP. Once you are diagnosed, an analysis of the family should be done to figure out if other family members have FAP. Genetic testing can find the abnormality and then see if other family members are also affected.
There are things you should think about when it comes to genetic testing. Tthink about how the results will affect you and your family members. Concerns may include what a positive or negative test means for you or others, passing the gene on to children, and challenges with employment and insurance matters. You should meet with a genetic counselor if you want testing. They are trained to help you understand the risks and benefits of testing and what to do with the results.
Treatment
Aspirin and some non-steroidal anti-inflammatory drugs (like sulindac and indomethacin) have been shown to shrink or reduce the number of polyps in those with FAP. A clinical trial studied the benefits of a targeted therapy medication called erlotinib with sulindac. Clinical trials continue to try find ways to prevent polyp growth.
People with FAP need to have their colons removed to prevent getting colon cancer. This surgery is often done when you are in your late teens and don’t have any symptoms of FAP. There are many surgical options. The goal is to remove all colorectal tissue at risk for polyps and to continue being able to pass stool through the anus.
Research about FAP has led to the availability of genetic testing for those at-risk, improved screening and surgical options, and clinical trials for the prevention of polyps. Continued research into FAP will lead to better treatments and outcomes. If you have any questions about FAP, you can always ask your providers or genetic specialists.
Resources for More Information
Learn more about surgical options for FAP, at the Zane Cohen Centre for Digestive Diseases/Mt Sinai Hospital, Toronto Canada.
Find a genetic counselor in your area.